How Caste Networks Influence ASHA Hiring, Obstructing Dalit Applicants
SC ASHAs from rural Bihar, Gujarat, Haryana, Maharashtra, Rajasthan, and Uttar Pradesh reveal how dominant caste networks obstruct the appointment of ASHA workers from marginalised communities, denying them opportunities to earn and lead

A CANAL CUTS OFF A HAMLET of around 65 households from the rest of Mathiya Bhakariya village in Kushinagar district in eastern Uttar Pradesh. These are the homes of the Musahars, among the most marginalised Scheduled Caste communities in Bihar and eastern Uttar Pradesh, who largely survive as agricultural labourers.
In this hamlet, Vimla Devi, 55, an Accredited Social Health Activist (ASHA), herself a Musahar, is the community’s primary link to basic healthcare. In 2007, Vimla, who dropped out after Class 8 from the local Hindi-medium school, became one of the first recruits under the National Rural Health Mission’s newly launched ASHA programme, tasked with connecting remote communities to the public healthcare system. She had found an application form for the post at a neighbourhood shop.
She was the last of her community to join the cadre in Mathiya Bhakariya. “No new Musahar ASHA was hired after me,” Vimla told BehanBox.
Data accessed from the Block Community Mobiliser of Padrauna block by BehanBox underscores this imbalance: of the 435 ASHA workers in rural Padrauna — which includes Vimla’s village — 261 are from OBC communities, 108 from the general category, and 66 from Scheduled Caste communities.
Vimla believes this imbalance is tied to the growing visibility and importance of the ASHA programme over the years. As the role gained social and financial value, more women from dominant communities began seeking it. And they are, she alleges, willing to pay a bribe of as much as Rs 50,000 to get the job. “I’ve heard people pay for these positions — to whom, I don’t know — but it is happening,” she says.
She argues that ASHA posts should be reserved for women from poorer and marginalised communities, not those with financial and social capital: “How can poor women from our community, or other marginalised Scheduled Caste groups, arrange Rs 50,000 just to secure the job?”
Under the 2013 revised ASHA Guidelines, the selection of ASHAs follows a multistep process developed through earlier guidelines and orders issued between 2006 and 2012. At the block level, the Block Community Mobiliser (BCM) and ASHA facilitators generate awareness about the role and responsibilities of ASHAs through community meetings and mobilisation events such as Kala Jathas.
With support from Panchayati Raj Institutions, women’s self-help groups, and other community organisations, facilitators organise meetings to identify potential candidates, shortlisting at least three women from each village. A Gram Sabha is then convened to select one candidate from the shortlist, with the proceedings and approvals formally recorded. The selected candidate’s name is forwarded by the Gram Panchayat to the Block and Nodal Officer for documentation. The District Nodal Officer, supported by the District Community Mobiliser, oversees the entire selection process.
One of the criteria for selection says: “adequate representation from disadvantaged population groups should be ensured to serve such groups better”. But in conversations with BehanBox, ASHA workers from Bihar, Gujarat, Haryana, Maharashtra, Rajasthan, and Uttar Pradesh reveal that the appointment of ASHAs has ceased to be procedural or transparent in recent years, largely affecting potential Scheduled Caste applicants.
This is the third and final part of our three part series on ‘Care and Casteism’, in which we document the lived experiences of Scheduled Caste ASHA workers within communities and the public health system. You can read the first and second parts here and here.
This series draws on a six-month-long investigation into caste-based exclusion among ASHA workers — an issue for which little official data or documentation exists. To understand its scale and impact, we conducted a micro-survey with 52 ASHA workers from Scheduled Caste (SC) communities across rural Bihar, Gujarat, Haryana, Rajasthan, Maharashtra, and Uttar Pradesh. The survey examined experiences of caste discrimination and its effects on access to work opportunities. [The methodology of the survey is detailed in the postscript.] In addition, we interviewed at least 10 ASHA workers from OBC and other communities whose accounts further informed this reportage.
[Scroll visualisations to explore data from the micro survey]
[Scroll right for the visualisations from the survey on Caste and ASHA workers: All visualisations by Urvi Sawant ]
Not All ASHAs Are Equal
Winning the support of the villagers and the approval of the mukhiya was only the beginning of a fraught recruitment process for Sharda Kumari, 42, a Scheduled Caste ASHA worker at Punpun Primary Health Centre (PHC) in Bihar’s Patna district. In 2006, she still had to battle fierce resistance from supporters of the seven upper-caste candidates who applied for the post.
“I got the job. Iss par hungama khada kar diya (all hell broke loose),” she recalls. “People assumed that the other, upper-caste candidates were more educated and thus more deserving than me. They opposed my appointment at every step. Mukhiyaji stood by me, but we were afraid it would turn violent.”

So tense was the atmosphere that she was afraid to even attend the first day of training and when she finally did, was barred from joining the session until the Gram Panchayat head stepped in on her behalf. Nearly two decades of work in the field have finally shifted attitudes, she says, largely because she “proved” herself through her work. As we reported in the first part of the series, SC ASHA workers had to work harder than their upper caste counterparts to earn the trust of their communities.
In her 2018 ethnographic study, Caste, Class, and Gender on the margins of the State, Madhumita Biswal documented how panchayat bodies and upper-caste health workers often worked consciously to block the appointment of SC ASHA workers. She writes of an instance in Odisha’s Baunsuni PHC, where an Auxiliary Nurse Midwife (ANM) described how caste prejudice overruled the selection process: “No Harijan woman is selected in our sub-centre area as ASHA. In one of the villages, a woman belonging to the Harijan caste had applied for the post. Though I was interested in selecting her, the village committee did not want a Harijan woman as ASHA. Hence, I could not do anything.”
Prerna*, an ASHA worker from Dudhola block in Haryana’s Palwal district told BehanBox how political connections derailed the appointment of a Scheduled Caste applicant. In 2013, Prerna, who is associated with the Centre of Indian Trade Unions (CITU), helped an SC woman apply for the ASHA post. She was selected and was due to begin training when she was abruptly informed that an upper-caste woman had been appointed in her place.
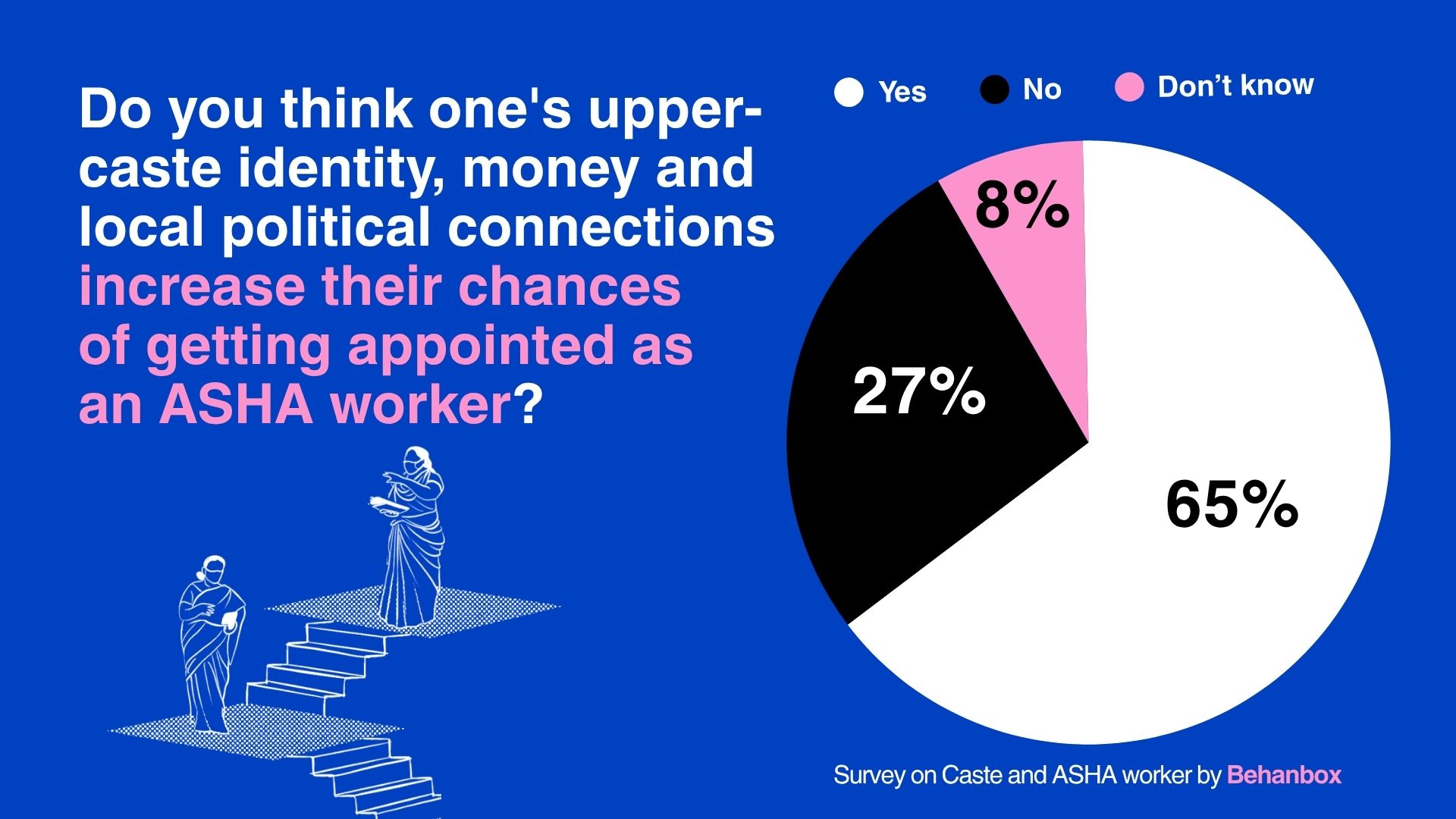
Up to 65% of the ASHA workers in our survey said that one’s upper-caste identity, money and local political connections determined their chances of appointment as an ASHA worker.
In Madhya Pradesh, Lakshmi Kaurav, an ASHA facilitator and State President of the Madhya Pradesh ASHA/ASHA Sahyogini Shramik Sangh belonging to a dominant caste among the Other Backward Castes (OBC), says upper-caste women often benefit from entrenched social and political networks that shape everyday village governance, giving them a clear edge in securing ASHA positions.
Lakshmi acknowledges that her own appointment, too, was eased by family connections: male members of her family who were active in the panchayat helped ensure she got the job.
“Beta, naukri karogi? Nurse ki? (do you want to work as a nurse?),” her chacha-sasur (father-in-law’s younger brother,) who was then the deputy sarpanch, had asked her. Lakshmi, who had once dreamed of becoming a doctor before being married off at 14, said yes instantly. To her, the ASHA job felt like the first chance to become something beyond the life already decided for her. She narrates her experience in an interview with us here.
“They knew about the ASHA vacancies through their connections in the panchayat,” Lakshmi told BehanBox. “The posts were quietly divided among their own daughters and daughters-in-law.”
Powerful Social Factor
The faultlines of caste in community healthcare had become apparent during other localised experiments. Caste, according to T Sundararaman, former Executive Director of the National Health Systems Resource Centre, was the main challenge in scaling up Chhattisgarh’s Mitanin programme, the precursor to the nationwide ASHA programme. It was, and remains a powerful social determinant that shaped who got selected, who was accepted, and whose authority communities recognised.
In the early years of recruitment, he said, social and political patronage often shaped ASHA appointments. Some workers were effectively “sarpanch-nominated” rather than genuinely “village-nominated,” and, in his words, the National ASHA Mentoring Group (NAMG) “couldn’t quite avoid that”. The NAMG, a technical and advisory body to support the Centre and states in implementing and monitoring the ASHA programme, was set up by the Ministry of Health & Family Welfare.
He pointed out that since the ASHA job was not desirable in the past as it is today, status alone did not determine the selection. He said that often the role went to someone within the sarpanch’s community who had limited social backing or needed institutional support. He argued that the gendered nature of the role also mattered: many women were seen as naturally suited to care work and responsibility in rural settings, where health work was not yet heavily commercialised. As a result, he said, the barriers were ultimately “not as much as we feared they could have been.”
There was another interesting aspect to ASHA recruitment in its early years, says T Suderraman: the turnout would be high but many who arrived with expectations of influence or authority dropped out quickly once they realised that the role offered little status and even lower remuneration than it does today. What followed was a second and then third cohort of workers, who have since stabilised the programme and remained in place for over 15 years.
In its last recorded meeting in October 2013, the NAMG flagged the need to strengthen the ASHA selection process. The meeting, co-chaired by Sundararaman, stressed that communities must have greater ‘control and ownership’ over selection, with explicit emphasis on ensuring representation of weaker sections among ASHAs. The minutes note the group’s concern that inclusion and transparency could not be left to the “state’s discretion only."
T Sundararaman said that while a strong sense of public service and altruism helped many ASHAs assert their agency and “move beyond barriers,” exclusionary practices cannot be ruled out. He added that the structural problems that shaped the programme’s early years still persist.
Both Sundararaman and Indu Capoor, former NAMG member and founder-director of the Ahmedabad-based NGO CHETNA, expressed frustration over the government’s reluctance to meaningfully engage civil society groups and NGOs in addressing on-ground inequities. They noted that NAMG proposals to strengthen such participation were turned down on the grounds that it would “undermine the role of the panchayats” — institutions that they argue are often dominated by entrenched caste elites.
Bribery and Exclusion
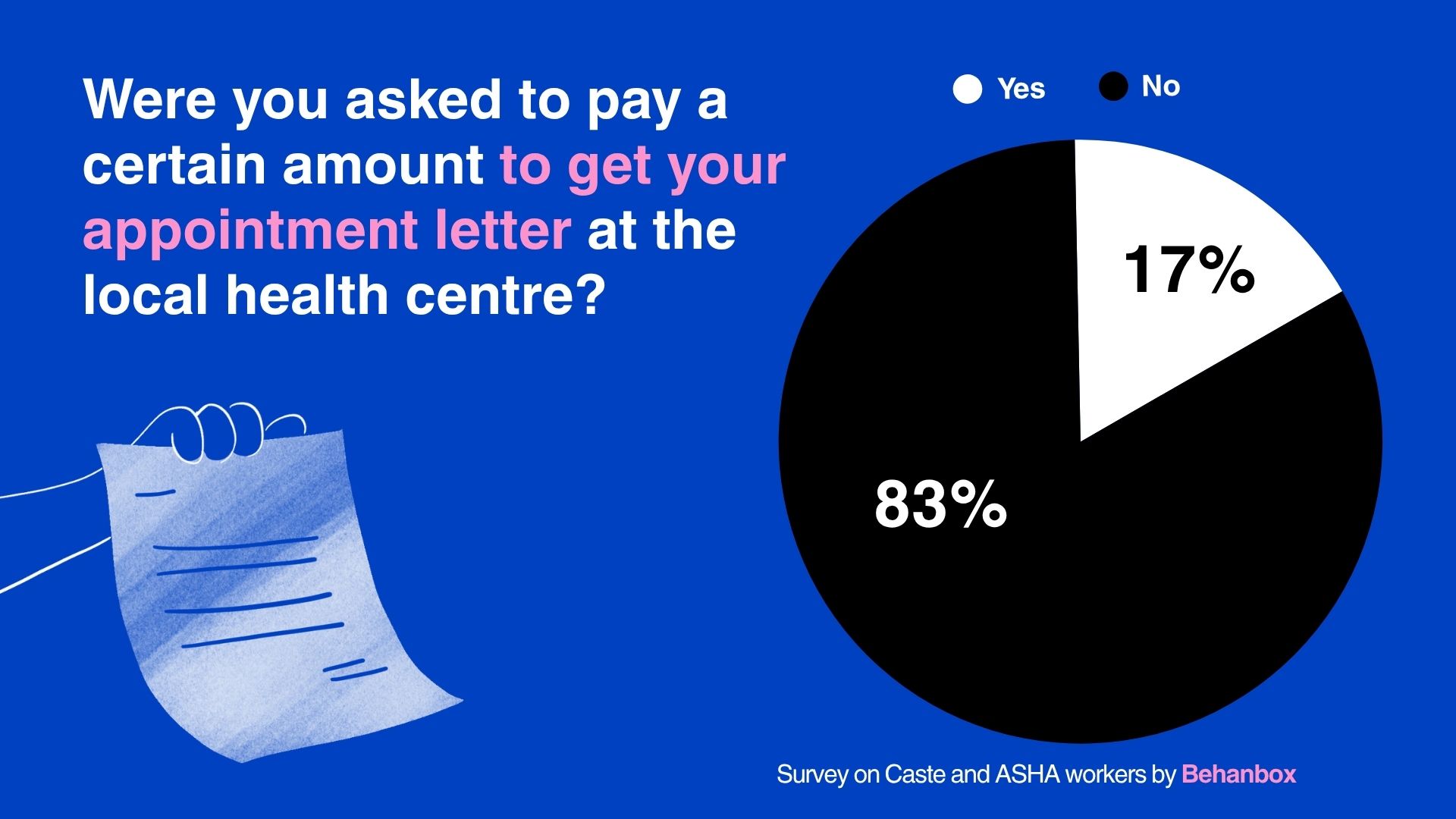
Sneha Kumari (name changed), a 33-year-old ASHA from Phulwari Sharif block in Bihar’s Patna district, says she had to borrow Rs 25,000 to bribe a data operator and Block Community Mobiliser (BCM) to obtain her appointment letter. She says she was misled into believing the post was a well-paying government job. Hoping for a stable income, and with her husband’s support, she applied and paid up.
Sneha reiterates that it has become increasingly difficult to find recently recruited ASHAs from Scheduled Caste communities in her block. As we detailed in part one of the series, government departments at the state and district level are uneven in maintaining official caste disaggregated data on the ASHA workforce, even though it is mandated by government guidelines. Those appointed between 2006 and 2010 allege that the earlier process of village-level selection has gradually been replaced by personal networks, commissions, and bribes.
“Even when forms are issued and SC women apply, they don’t get selected because everything is already decided by the mukhiya,” she says. “Earlier there were more SC ASHAs, but most of them are now older. Today, there are more OBC and general category ASHAs because they can afford to pay the money.”
Earlier, SC applicants were prioritised during hiring, she recalls. “But now upper-caste women see that we are earning from it, so they bribe certain authorities and get the job instead. Where will poor people get Rs 10,000 to Rs 50,000 from?” She adds that even workers at the PHC demand money to issue joining letters.
In Sampatchak block, near Phulwari Sharif, Soni Kumari, an OBC ASHA worker, recalls being asked to pay Rs 50,000 by a Primary Health Centre (PHC) staff member in exchange for her appointment letter. Her mother had already managed to arrange Rs 20,000, hoping it would secure a source of income for her daughter. In the end, however, Soni received the appointment without paying. She notes that the village mukhiya, who also belonged to her community, may have worked in her favour.
Lakshmi affirms the allegation of corruption. In Madhya Pradesh, she says, it is “very rare” for an ASHA worker to be appointed without a bribe of Rs 10,000-Rs 15,000 being paid to the panchayat members or officials who process the applications.
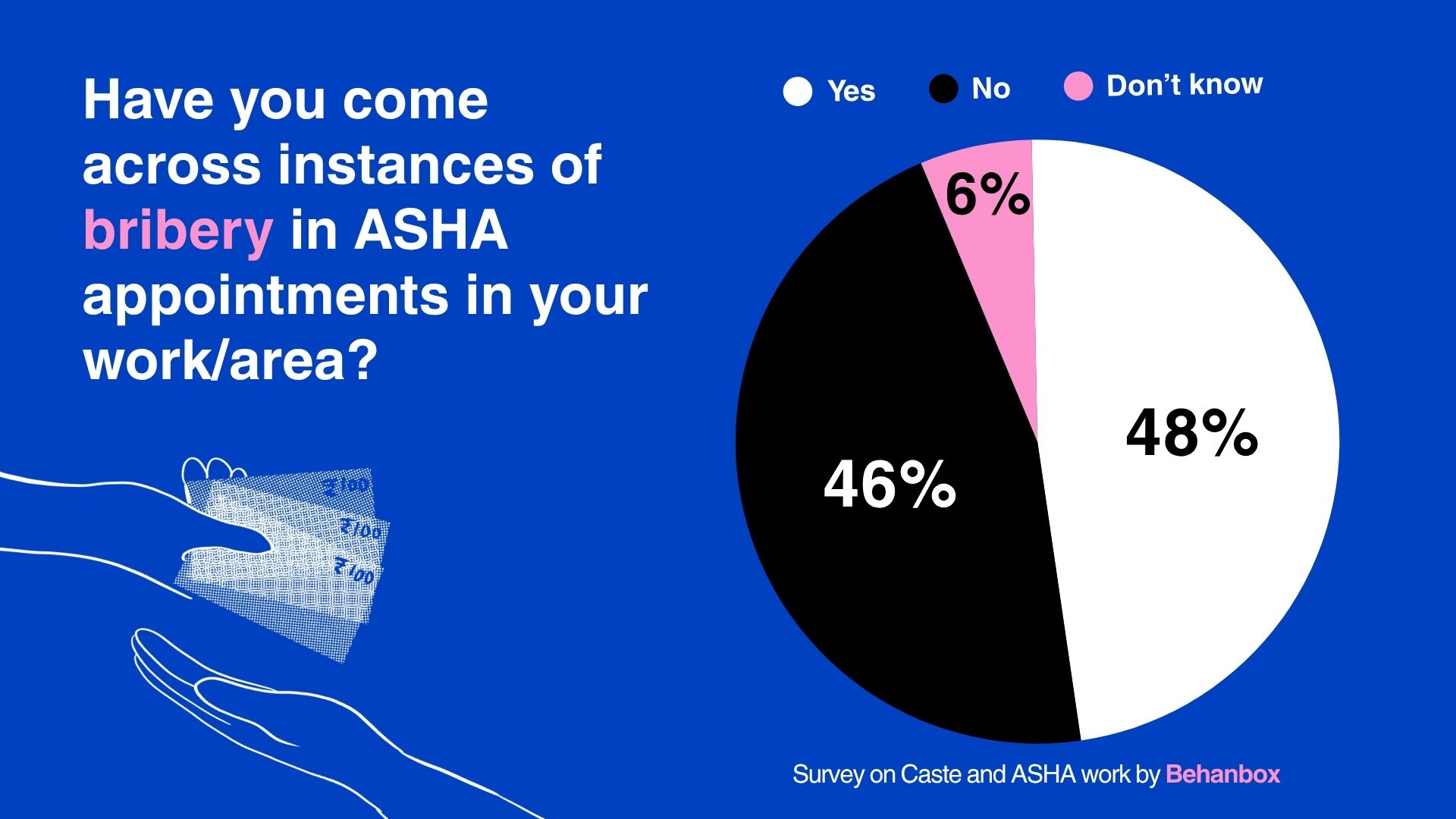
At least 48% of the ASHA workers in our survey said that they are aware of at least one case of bribery in the ASHA appointment in their block. Around 17% said they themselves were asked for money to confirm their selection.
T Sundararaman said bribery was not an issue the NAMG encountered in its meetings between 2009 and 2013, largely because the Janani Suraksha Yojana was the only functional performance-based incentive at the time. However, he added that such practices are not implausible today, given that ASHAs now earn around Rs 5,000– Rs 6,000 and the programme has gained both popularity and social respect.
“There has to be zero tolerance for this. There are no mitigating measures,” he says. “If the programme is taking bribes of this value, there is no question it has lost its way.”
Dharmishtha Chauhan, an SC ASHA facilitator from Nana Kalodra village in Gujarat’s Anand district, says ASHA posts are now coveted by upper-caste women and this has changed attitudes to recruitment. “Earlier, women had to be encouraged or called to apply. Now they come on their own asking, ‘If any ASHA is being removed or leaves, let us know. we will join,’” she says.
Commenting on the systemic exclusion of the most marginalised women from the community healthcare programme, Indu Capoor says the initial hiring process was “very participatory and transparent,” but added that the gaps at the community level were not fully visible at the time.
“You can design a very good system, but what happens at the village level is driven by politics—and caste politics is the biggest force,” she said. “A woman sits at the lowest rung of that hierarchy. Everything we did with good intentions somehow got distorted through jugaad (hack) at the grassroots level.”
Social Networks and Parallel Incentives
Even as caste and class dynamics exclude Dalit women from recruitment, those already appointed say their earnings and incentives are impacted by these same factors. Although no quantified dataset captures this, field reporting indicates clear patterns in how caste hierarchies operate on the ground to limit opportunities for those without social capital.
Varsha Marwari, an ASHA worker from Petlad block in Gujarat’s Anand district, says upper-caste families in her village often insist on calling ASHAs from their own community for institutional deliveries.
“Because they are from the same communities, those ASHA workers end up getting the incentives, not me,” she says. “The same happens with children’s vaccinations. They don’t trust me when I call them for immunisation, but they do trust their own acquaintances.”
In Musahar Tola, persuading residents to obtain identity documents like Aadhaar cards and open bank accounts has long been a challenge for Vimla. As a result, many deliveries take place at home, affecting her incentives due to incomplete paperwork. In contrast, upper-caste ASHAs working in relatively well-off areas are less likely to face such barriers, benefiting from higher awareness and the advantages of caste and class privilege.
“Discrimination has not ended; it has only changed form,” says Durga. “You never know when or how your entitlements will be taken away. Most households don’t survive on ASHA income alone. Very few are fully dependent on it. But SC ASHAs often are—it is their only source of income,” says Durga, a community activist from the Musahar community in Kushinagar.
When An SC ASHA Worker Decides To Lead
Roshni Devi* from Sampatchak block in Bihar’s Patna district has worked as an ASHA since 2006. She says she has never faced discrimination in the field on account of her Ravidas or Scheduled Caste identity. It was only in 2023, after a Centre of Indian Trade Unions (CITU) representative observed her work and communication skills and appointed her vice president of the group, that she says she encountered discriminatory behaviour from some of her own colleagues.
“Ek chhota jaat ka aadmi, wo kaise upadhyaksh ban gayi hai (how can someone from an oppressed caste become vice president)?” she recalls them saying. “We will not keep her in the union,” some members from upper-caste communities reportedly said.
The opposition surfaced in multiple ways—from limited acceptance of her leadership to outright neglect and social exclusion. The CITU representative who had supported her election also came under pressure from other ASHAs. As a result, Roshni stopped being informed about meetings, demonstrations, and other union activities. Isolated and without support from her colleagues, she eventually felt compelled to step down.
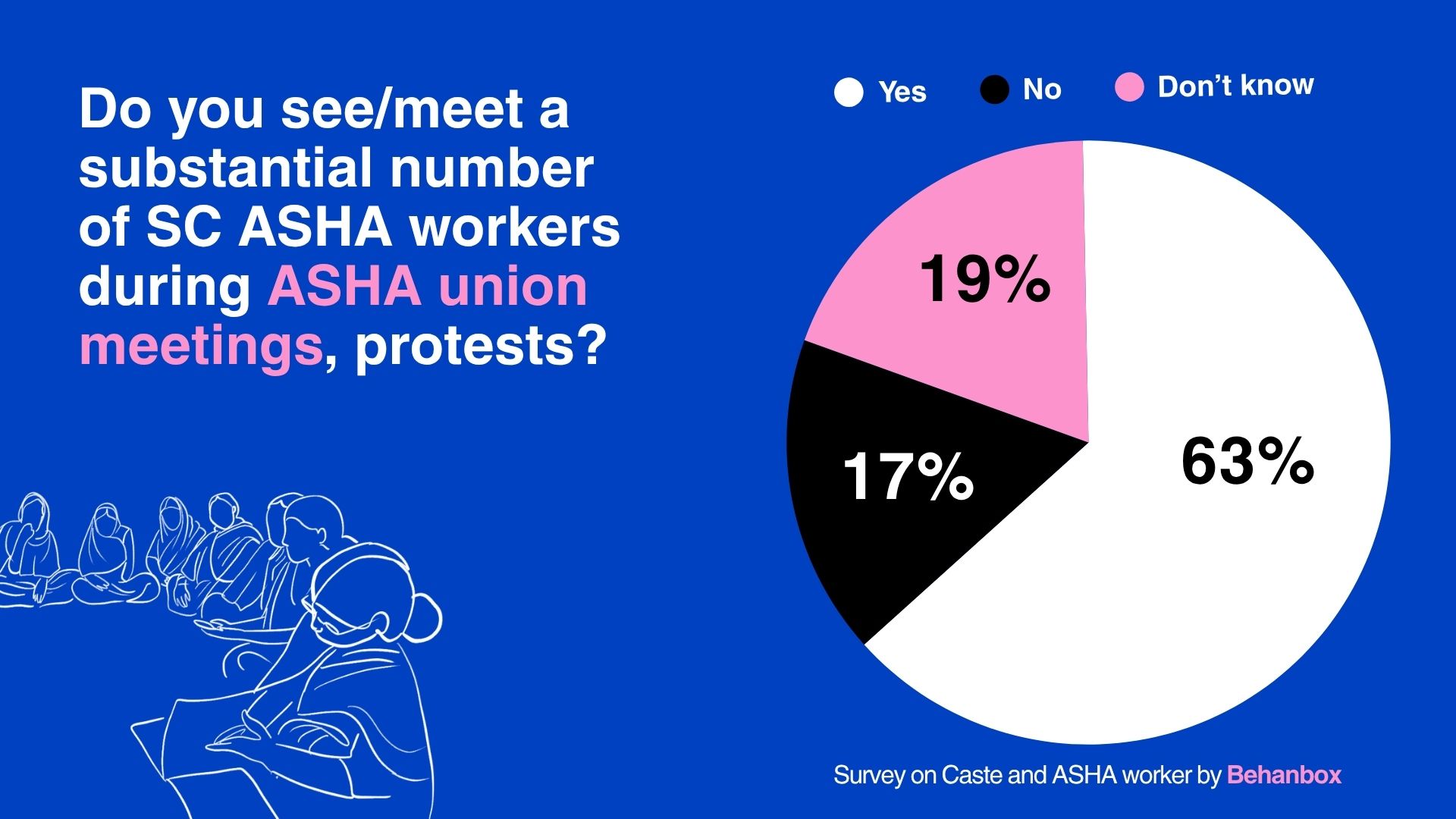
On the other hand, ASHA union leaders from OBC and upper-caste communities acknowledge caste bias within the system, and note that their unions do include SC ASHA leaders. However, they also say there is limited scope to address casteism among ASHA workers themselves. At least 63% of the ASHA workers we surveyed said they see a substantial number of SC ASHA workers during ASHA union meetings or protests, yet 67% of them stated that the issue of caste discrimination does not figure in such gatherings.
Netradipa Patil, ASHA worker belonging to the dominant Maratha community and State President of the ASHA Workers’ Union under the Bharatiya Bahujan Majdoor Sangh in Kolhapur, says that leadership selection within their union is guided by the principle that candidates should not carry “caste pride.”
“There are many ASHAs who are Dalits, and they should feel represented at a larger stage,” she says. “We try to be as inclusive as possible across communities in leadership positions. For example, our sah sachiv (secretary) is a Dalit from Nanded district, while the president is from an upper caste.”
Leadership roles within union groups remain a distant prospect for many SC ASHA workers, and even the position of ASHA facilitator comes with significant challenges.
‘They Asked For Proof Of Prejudice’
In Haryana’s Palwal district, Prerna was forced to resign from her role as ASHA facilitator in 2024 after prolonged harassment by block coordinators at the Community Health Centre (CHC). A district president of the Centre of Indian Trade Unions (CITU), she has been actively campaigning for ASHA workers’ labour rights since 2009.
She says her activism and leadership drew hostility from CHC coordinators, who began withholding her payments and incentives and, she alleges, made casteist remarks such as, “neechi jaati walon ko naukri mil jati hai toh zyada hi bante hai (when lower caste people get jobs, they start acting too proud)”.
As an ASHA facilitator, Prerna worked long hours, covering 29 villages in 15 days, managing vaccination camps, coordinating with around 60 ASHAs, verifying proformas across 74 tasks, and compiling reports. She says repeated letters to authorities, including the Chief Minister’s Office, only led to prolonged discussions marked by dismissive remarks. Even after offering to produce proof of her work, she eventually received her payment, but with significant deductions.
“I complained about the casteist remark, but they asked for proof,” she says. “The general category ASHA worker who witnessed it did not support me. No one was able to do anything.” She adds that she also chose not to raise it further with other ASHAs: “They already look up to us, and I didn’t want to discourage them. We may think we are equal, but we are reminded otherwise in different ways. Even today, this continues.””
Eventually, she stepped down from the facilitator role and now works only as an ASHA.
Development economist Srujana Boddu notes that caste identity and hierarchy often operate through “internal or hidden mechanisms” that shape how power is distributed within groups that may otherwise share common demands.
Roshni and Prerna’s stories show how caste influences who gets to speak, who negotiates, and who ultimately benefits from leadership positions. These internal hierarchies, Srujana argues, “cannot be ignored, as collective bargaining may remain uneven and fragile, and end up reproducing inequalities in one form or another.”
Although Roshni Devi was elected as a union leader, she was not treated as one. Over time, she was pushed to the margins through exclusion from meetings and decision-making spaces, eventually limiting her participation. This, despite her consistently raising issues that affected all ASHA workers, regardless of caste.
“I joined the organisation to fight for everyone’s rights, but they saw my caste, not my abilities as a leader,” Roshni says. “I wasn’t fighting for myself alone—the union is for everyone. You cannot oppress anyone from that position. For me, everyone is equal.”
The data behind this investigation comes from a survey of 52 SC ASHA workers across six states: Bihar, Gujarat, Uttar Pradesh, Haryana, Rajasthan and Maharashtra. To request the cleaned dataset for research, advocacy or reporting, fill this form.
A brief note on the survey methodology
The survey was conducted with 52 ASHA workers from SC communities across 6 states– Bihar, Gujarat, Uttar Pradesh, Haryana, Rajasthan and Maharashtra. The survey was conducted both in-person and through telephonic interviews. We surveyed 13 SC ASHA workers on the field and 39 on the phone.
The survey had 19 questions. These included their demographic, education and caste details. The questions on the experience of casteism within the healthcare system included instances (if even one time) of caste discrimination, detailed narration of the experience, institutional support mechanisms, questions on bribery and favoritism, opportunities and upward mobility, mental health effects and spaces within the labour unions. These responses were then converted to variables and analysed.
One major shortcoming of the survey is that it was conducted in Hindi speaking regions, leaving the entirety of South India and many other states due to resource constraints. We hope this is a start into a longer research and inquiry into the caste question in other states.




We believe everyone deserves equal access to accurate news. Support from our readers enables us to keep our journalism open and free for everyone, all over the world.
