20 Years On, Dalit ASHA Workers Are Fighting A Lone Battle Against Caste
A community healthcare programme cannot be immune to the injustices of a casteist society. Amid lack of institutional support and refusal to make it a part of union struggles, Dalit ASHA workers recount experiences of discrimination on the field

In 2012, Rekha, a 34-year-old Accredited Social Health Activist (ASHA) from a Scheduled Caste (SC) community, was posted in Sihol, a predominantly upper-caste village in Petlad block of Anand district in Gujarat. She was an accomplished health worker with a higher secondary education and, in the words of her immediate supervisor — the Auxiliary Nurse Midwife (ANM) — a fast learner deeply committed to community care. Yet, despite her competence and dedication, it was her caste that shaped the perceptions of her ability to provide care.
“You are a Harijan. Your position is outside my house. Finish your work at the door,” she recalled being told by a member of a Patel family, the dominant caste community in the village. Rekha had gone to their home to check a newborn’s weight, one of the main tasks of an ASHA worker. Just the day before, she had accompanied the mother to the hospital for delivery.
The incident is not without irony. Many years earlier, Rekha’s daadisaas (grandmother-in-law), a daai (midwife), had helped deliver a baby in the same household. Rekha’s experience both hurt her and left her enraged.
“They treated me with disrespect. So I stopped going to their house,” she told BehanBox. She asked the family to come to the primary health centre instead if they needed health care.
Rekha’s experience is far from unique. Across interviews that BehanBox conducted with ASHA workers and facilitators from the SC and also from OBC communities, as well as union leaders, we found that accounts of caste-based discrimination ranged from overt exclusion and untouchability to more covert, everyday forms of prejudice.
As part of our six-month long investigation, we undertook a micro-survey to understand the scale of exclusion and prejudice, as very little data and documentation on this issue exists. We spoke to 52 ASHA workers from SC communities across a range of issues – instances and experiences of caste based discrimination, institutional support systems, spaces within labour unions – in rural Bihar, Gujarat, Haryana, Rajasthan, Maharashtra and Uttar Pradesh. [We have detailed the methodology in post script.]
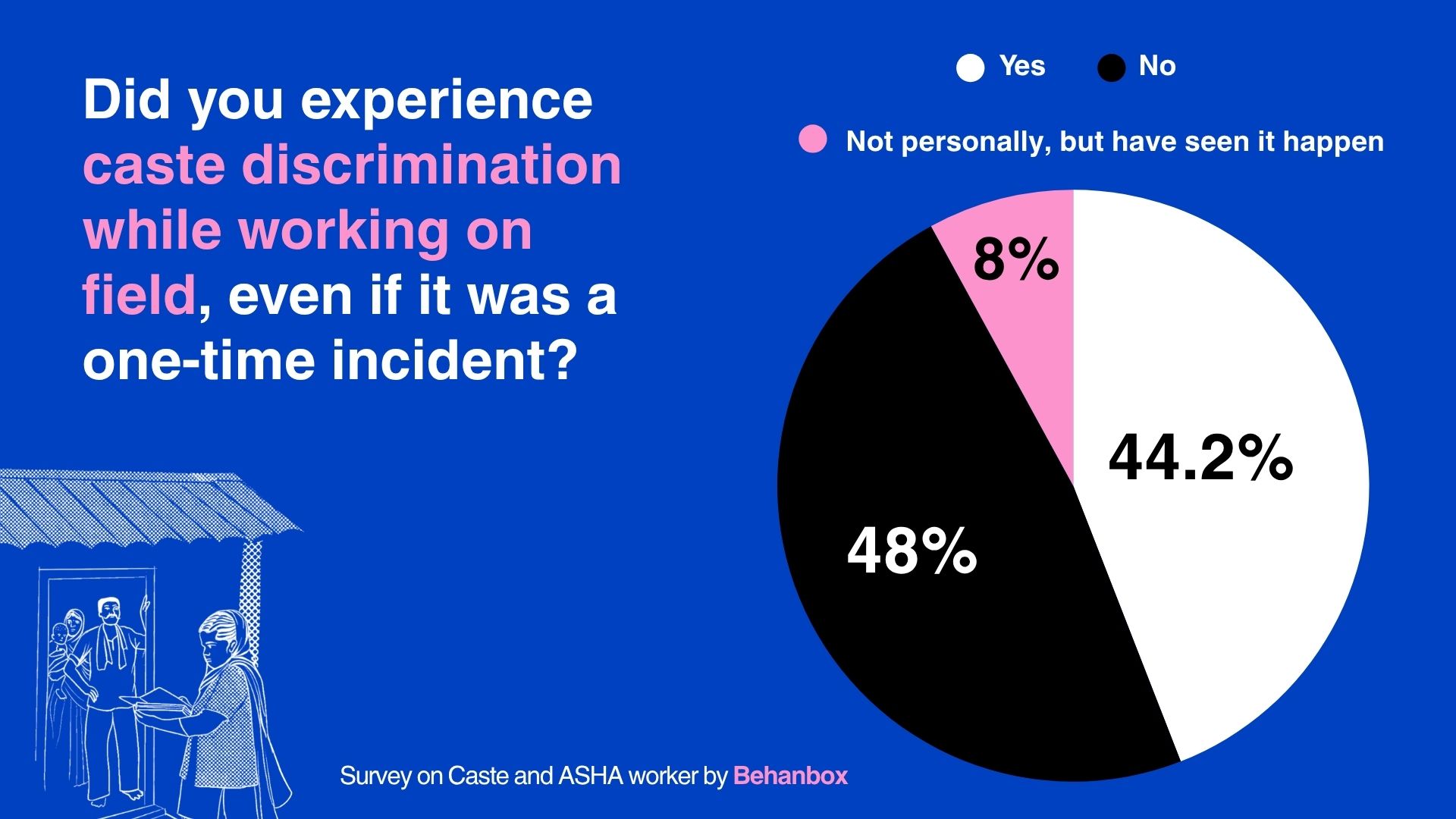
Our survey threw up significant insights. Around 48% of ASHA workers reported to have been explicitly asked about their caste identity during their initial interactions with the community. At least 44% reported having faced discrimination at least once in their work by village residents, while 7.7% said that they had seen it happen to others even if they did not experience it first hand.
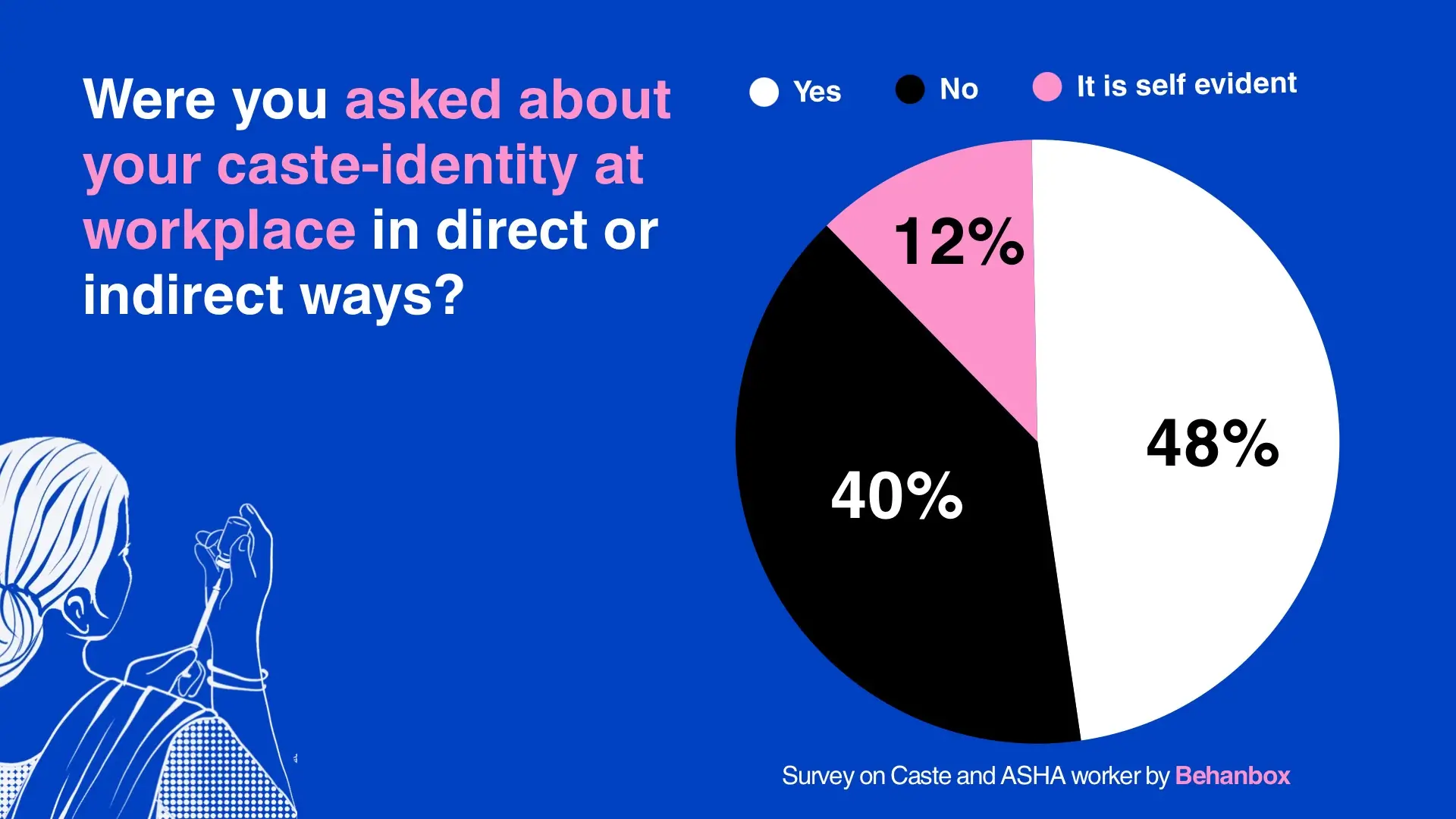
[Scroll right for the visualisations from the survey on Caste and ASHA workers: All visualisations by Urvi Sawant ]
This is problematic not only because it amounts to workplace injustice, but also because it undermines community healthcare delivery and erodes the morale and dignity of ASHA workers. We found that they face multiple levels of caste-based exclusion – from their peers, the communities they serve, the healthcare system and even the unions they are a part of.
Since 2005, ASHA workers have been the essential bridge between local communities and the public healthcare system, fulfilling basic community health needs – maternal and child health, pre- and post-natal care, and adolescent health along with other functions. In recent years, their tasks have expanded to include government surveys and even election and Census duties. But despite this, ASHA workers are labelled “volunteers”, paid honorariums far below minimum wages and denied basic employment benefits, as we have reported. In the last 20 years, ASHA workers have been protesting this exploitation and the denial of basic labour rights and decent work conditions.
The question of caste, however, has remained in the shadows both in official rules of conduct as well as within the labour rights movement led by the ASHA workers themselves. To understand this gap, BehanBox, through a three part series, has undertaken to document the lived experiences of Scheduled Caste ASHA workers within communities as well as in the public health system.
In the first part of the series, we interviewed Dharmishta Chauhan, an ASHA facilitator from Gujarat, whose experience of caste and disability shapes her care work. This, the second article in the series, documents the many ways ASHA workers face caste indignities while providing care and how they resist. The third and concluding part will look at how caste hinders their appointment and upward mobility within the healthcare system as well as the unions.
This series of stories is part of our feminist historiography project – The ASHA Story – that seeks to document the lives, labour and expertise of India’s 1 million ASHA workers. And to our knowledge, this is the first micro-level data exercise that foregrounds caste in examining ASHA workers’ experiences within India’s healthcare system.
Up Close With Caste Hierarchy
In less than two decades, ASHA workforce has grown nearly tenfold — from 140,000 to over one million. They have played a pivotal role in arresting maternal and infant mortality across India and during the COVID-19 pandemic, they were central to India’s disease response and vaccination drive. For this, their work has been honoured by the World Health Organization with the Global Health Leaders Award in 2022.
But in a deeply caste-stratified society, we found that an ASHA worker’s caste identity — often immediately known — frequently determines whether the community accepts her care work, and on what terms. Rekha’s caste was uncovered in less than six months of her joining her job at the Petlad PHC. Once it was revealed that she was a ‘Harijan’, things began to unravel. One day, a woman from the upper caste community who had regularly interacted with her abruptly stopped speaking and began keeping her distance.
“I should get some respect. I am working for the government after all,” said Rekha.
In Nana Kalodara village, 30km away, dominant caste villagers repeatedly tried to have Varsha Marwari, another Scheduled Caste ASHA worker, removed from her job. They lodged false complaints alleging that she had failed to conduct house visits. In response, she began meticulously documenting every visit she made.
“When I was informed about the complaints by my seniors at the Community Health Centre (CHC), I started keeping receipts in the form of photographs, and signatures in my ASHA diary for every visit,” said Varsha. The complaints stopped.
For ASHA workers from marginalised communities, caste hierarchies and prejudice compound the already difficult conditions of frontline healthcare work, particularly in rural and semi-urban India. Yet these experiences remain poorly documented and understudied. There is also little publicly available data on the caste composition of ASHA workers and ASHA facilitators across states and districts. Under the 2013 ASHA guidelines, block and district nodal officers are required to submit a consolidated ASHA database to the state health department annually. The database includes details such as an ASHA worker’s name, village, education level, caste, and date of selection, among other information.
In November 2025, this reporter filed Right to Information (RTI) applications with the health departments of Bihar, Gujarat, and Uttar Pradesh, seeking caste-wise and other categorised data on ASHA workers from districts covered in this reportage. Bihar and Uttar Pradesh failed to respond even after appeals were filed. Gujarat responded to the first appeal and transferred the request to the relevant district officer, but the data is yet to be provided. Many local health departments said that they did not maintain caste disaggregated data of ASHA workers.

‘I Am On Duty, Holding Your Baby’
In Phulwari Sharif block of Bihar’s Patna district, settlements are sharply segregated along caste lines. The contrast is apparent– well-built, painted homes of upper-caste families stand on one side, while Scheduled Caste households are pushed into isolated clusters deep inside the fields, far from the pucca roads. In rural India’s entrenched caste order, ASHA workers from marginalised communities are acutely aware of how their caste identity shapes — and often constrains — their work in the communities they serve.
Sneha Kumari*, a 33-year-old ASHA worker from the Ravidas community, shares an incident in a Rajput dominated village where she was mistaken for an upper caste person due to her light skin while her OBC colleague was taken to be an SC. “At times, they would sprinkle water if one of my colleagues touched their doors,” she recounted. The ASHA worker declined to do survey work and asked the seniors to assign her other duties.
Sneha had always been vocal about her caste. “I am a Ravidas – a Chamaar,” she would declare. She recalls an incident where a Rajput community member asked her if she was an ‘achhoot’ (untouchable), she shot back– ‘If I cut myself, does my blood say that I am Chamaar and yours Rajput? We have the same red blood, don’t we?’

Suman, an SC ASHA from Gorakhpur district of Uttar Pradesh, recalled that she was not allowed to sit on a chair during an immunisation house visit in Korari village. “I am on duty. I am holding your baby to administer the vaccine,” she reminded the family but they did not budge.
Sonara Alaji, an ASHA worker since 2020 from Dhandoka taluka in Ahmedabad district, Gujarat, tells us that affluent families do not take SC ASHA workers for institutional deliveries. It is mandatory for an ASHA worker to accompany a pregnant woman for institutional delivery–a precondition for her to receive her incentive under Janani Suraksha Yojana (JSY), a Central scheme for promoting institutional deliveries to reduce maternal and infant mortality.
“For regular checkups post-delivery, they never let us in after the third day. I do not go to their home, I just call up and check,” said Sonara. Things have somewhat improved, she reckoned, but the barriers to entry within homes persist.
Lakshmi Kaurav, an ASHA facilitator and Union leader from Madhya Pradesh, has seen this discrimination play out often in the field. Herself from the OBC community, she said that SC ASHAs are either not allowed to enter homes and if they do, not allowed to touch newborn babies. She has observed this discrimination especially in areas dominated by the Thakur and Brahmin communities.
“In upper caste homes, a woman who has just delivered a baby is deemed impure, especially by women of the household. It’s the only time when Dalit ASHA workers are allowed in to do their duties as both are considered ‘impure’,” she said. She noted that even an upper caste ASHA worker would hold the new mother as “impure”, reinforcing the notion of ‘purity’. In many households, said Lakshmi, even today, irrespective of caste, families do not allow any ASHA worker to touch the newborn.
When Need Blurs Caste Lines
Yet, there is a deep contradiction. While these notions of ‘purity’ persist on one hand, upper caste communities do not hesitate to reach out to SC ASHA workers, when it comes to other healthcare services. Srujana Boddu, a development economist at SRM University in Andhra Pradesh who has researched on care work and caste, explained this as a “negotiation in times of need”. The “need for care”, she observed, results in blurring of the rigid boundaries of caste. In that particular moment, an ASHA worker is a “service provider”. This does not erase caste or indeed, dismantle the caste hierarchy entirely.
“An ASHA worker will be accepted not as an equal, but probably be looked at as a service provider whose role is very conditional and instrumental here,” Srujana told BehanBox. Even during this moment of need, the boundaries are well understood by the worker as well as the receiver of the service or care. But once the immediate need passes, that discrimination, the distance will probably assert itself again.
The usual modes of discrimination–separate tumblers, plastic for Dalits and steel ones for upper castes– often seen in caste driven rural India also extend to ASHA and other care workers.
Official structures and mechanisms are either silent or inadequate in dealing with questions related to caste discrimination. The Ministry of Health and Family Welfare (MoHFW) set up the National ASHA Mentoring Group (NAMG) as a technical and advisory body to support the implementation and monitoring of the ASHA programme. In 2008, the National Health Mission (NHM) released Module 5 of the seven training modules developed by NAMG, focusing on values, communication, and leadership skills for ASHAs. It highlights self-respect, the importance of recognising threats to an ASHA’s dignity, and strengthening her agency as a frontline health worker.
While the module promotes non-discriminatory practice, it does not address what happens when ASHAs themselves face caste-based discrimination, or what safe and accessible remedies they can access. Similarly, NAMG meeting records from 2006 to 2013 emphasise the need for stronger institutional support, supervision, and pathways for ASHA advancement, with a broader focus on agency-building and social determinants of health. However, they do not lay out concrete measures to respond to caste-based challenges faced by ASHAs in rural settings.
Building Trust And Gaining Respect
In the absence of institutional support, over time SC ASHA workers learned to adopt their own methods to navigate the caste-driven indignities. Most Dalit ASHA workers refuse to drink water or use the furniture in upper caste homes until offered. Rekha refused to attend to those who disrespected her while Sneha Kumari was quick with retort to insults. Over time, ASHA workers say, the intensity of discrimination has somewhat eased. Many tell us that this is, in large measure, due to the commitment and care that ASHA workers have shown.
“We have built that kind of trust among the people. They know that we are available at all times, even in the middle of the night, if they need us,” said Rekha.
Lakshmi Kaurav believes that the caste indignities faced by ASHA workers have actually increased their resolve towards community care and they also come better prepared for meetings. This drive, she said, is missing among upper-caste ASHA workers who come with a sense of entitlement.
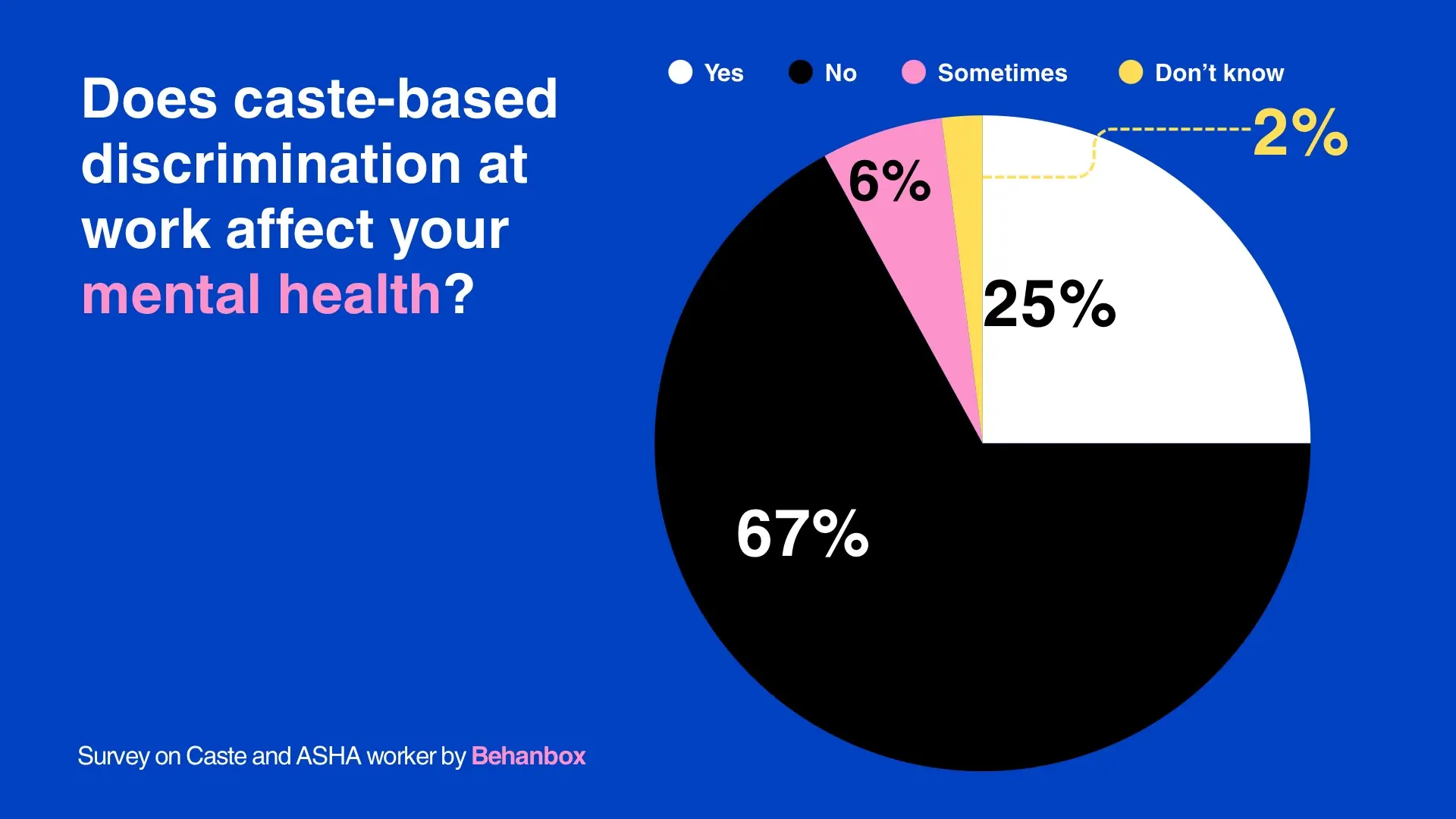
But this has come at a cost – the memory of indignity that refuses to leave. Upto 31% ASHA workers in our survey said that this has affected their mental health in multiple ways. "Bura toh lagta hi hai, pehle zyada lagta tha ab itna farak nahi padta. [It does not bother us as much as it once did, but it did hurt]. Also, they even respect us now,” said an ASHA worker.
Srujana observed that even when need forces upper caste communities to ignore caste, it adapts and reorganises in ways that allow them to extract care and labour without granting any recognition to the ASHA worker. “That’s how the system and caste work. It permits dependence without any dignity,” said Srujana.
Staying Quiet, For Fear Of Dismissal
Suman Kamble, 48, an ASHA worker in Chandgad taluka in Kolhapur district in Maharashtra since 2009, says that she faced ‘harassment’ from the Auxiliary Nurse and Midwife (ANM), her immediate supervisor. She was one among the four ASHA workers in the village–one Muslim and two Marathas.
“The ANM withheld information from me, complained to the authorities over minor mistakes, even if I was a little late,” she alleged. “She made me do her household chores – clean packs of chillies and rice, and wash her utensils. I was scared of losing my job so I kept quiet. There were no other work opportunities.”
The 2014 guidelines for monthly meetings of ASHA at Primary Health Centres (PHCs) and Sub-Centres, published by the MoHFW, notes that medical officers convening ASHA meetings are required to address problems raised by ASHA workers. In reality, not all ASHA workers from marginalised communities feel comfortable discussing caste discrimination with those governing daily functions at the health centre due to fear of being dismissed.
Suman Kamble narrated another incident where she was asked to make poha for some visiting officials from the health department. When she confided about this with her ASHA peers, they asked her to simply comply without protest.
Madumita Biswal, Assistant Professor at the Department of Sociology, Sambalpur University, discussed this in her paper where she explains how ANMs, Anganwadi Workers, and Multi-Purpose Health Workers, contribute in their own way to strengthen caste structures – upper caste women, she wrote, are brought in as agents of development while lower caste women enter the discourse as “governed bodies and objects of surveillance".
Suman feared losing her patients after the ANM tried to reassign them to others. Apart from affecting her incentives, this also meant that her patients stopped getting in touch with her about their issues. Her complaints to the doctor, also an upper caste, went unheard, she said.
“I was standing up to all of them alone but then I was silenced. I feel very distressed about it even today, and this affects my work too,” she told BehanBox.
Amod Kumar, an expert within the NAMG, shared his concerns about this ‘rude behaviour’ of the nurses and ANMs in the last and the 11th meeting. He expressed the need for sensitisation of the system’s functionaries and to develop a module for this.
T Sundararaman, former executive director of the National Health Systems Resource Centre, noted that ANMs, Anganwadi workers, and ASHAs were originally envisioned as a coordinated team with clearly defined roles and responsibilities. He explained that issues unresolved at the local level were meant to be escalated to ANMs, but in practice this rarely happened. Instead, concerns were typically pushed up to the PHC, making its doctors the de facto first point of reference.
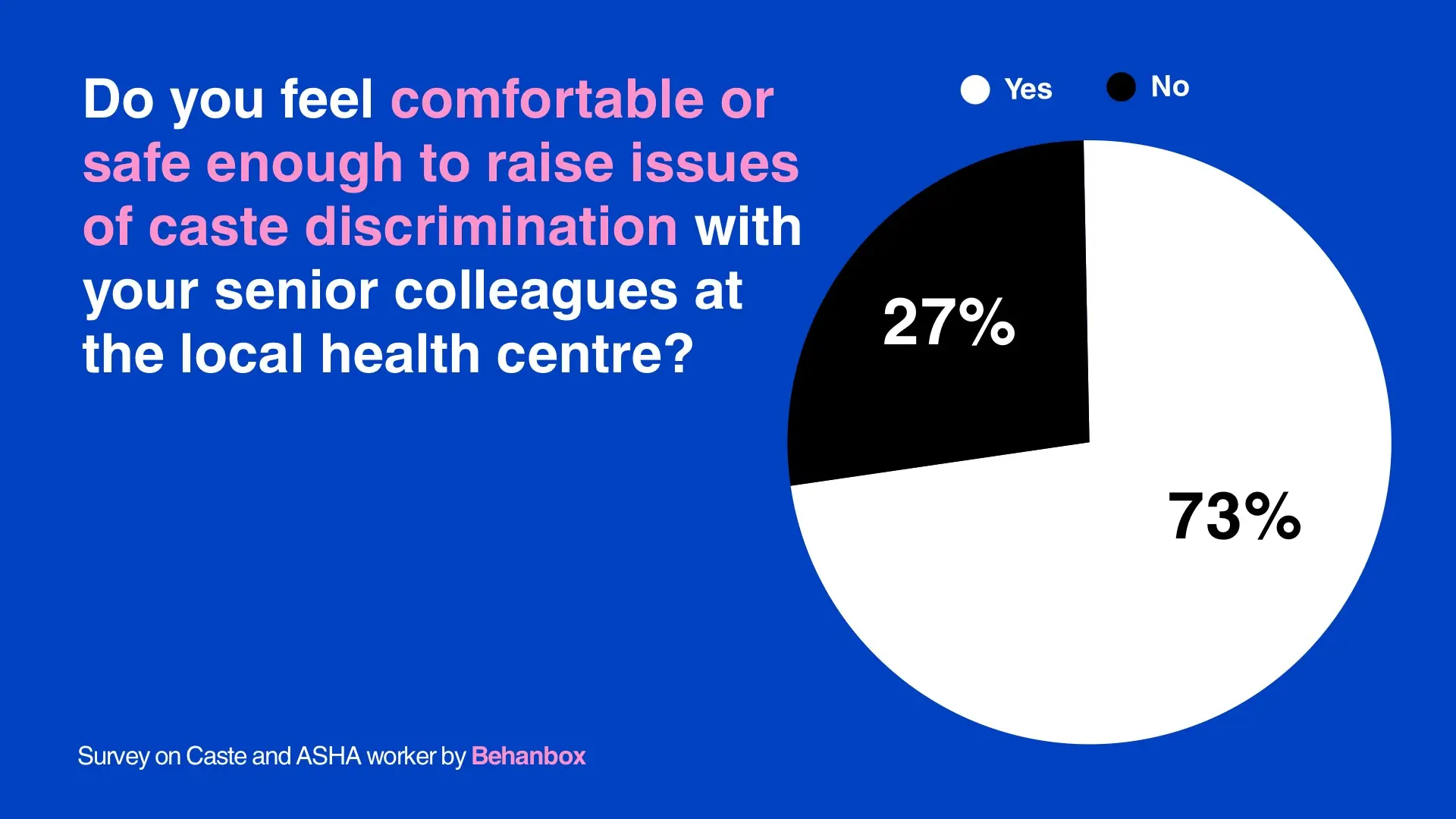
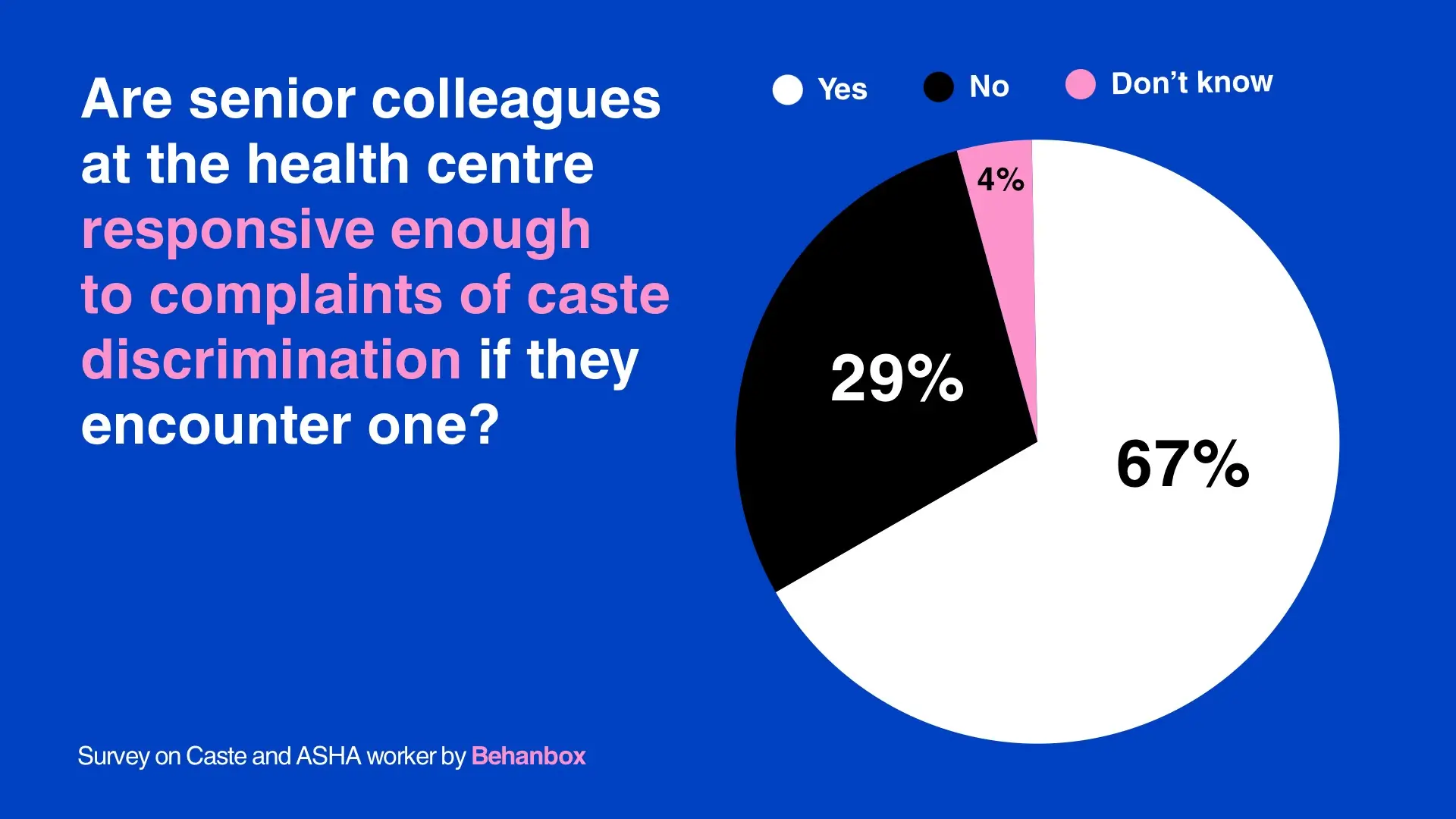
On the ground, however, such supervisory and facilitation structures have failed to address and create safe spaces for ASHA workers. When asked if they felt safe to discuss issues of discrimination with their seniors, 27% of ASHA workers in our survey said they did not and 29% said that senior colleagues, doctors and ANMs at the health centre are not responsive to their complaints about caste discrimination.

Parvati Verma, a Scheduled Caste ASHA worker from Jagatpura in Rajasthan’s Jaipur district, recalled that her concerns were initially ignored by senior staff, while ASHAs from other communities were treated “gently and politely”. When she raised a complaint with the community health officer about a doctor discriminating against people during a vaccination drive, she faced backlash from her peers.
Although the issue was eventually resolved, she alleges that was later transferred to another area following false complaints by the same doctor. “Even ASHAs from my own community stopped talking to me. Then I thought, Taalab mei rehke, magarmachh se bair karna kya [why pick a fight with the crocodile, when you have to live in the pond]?” she said.
Netradeepa Patil, an ASHA union leader from Kolhapur who belongs to the dominant Maratha community, corroborated this. “ANMs and other staff feel, ‘Kya karlegi woh (what can she do?)?’ Who will support her?’ But they will think twice before saying anything disrespectful to me,” said Netradeepa, the state president of ASHA workers Union, Bharatiya Bahujan Majdoor Sangh.
Sneha Kumari from Bihar said that the monthly meetings fail to make space for caste related conversations because they are led by upper caste ASHA workers who do not even recognise caste as an issue. Even those who do, keep silent for fear of backlash.
In Khambhat, Dharmishtha Chauhan, the first Scheduled Caste ASHA facilitator in her village, has worked to encourage her team of nine ASHA workers, including Varsha Marwari, to resist discriminatory practices. Having experienced caste discrimination during her time as an ASHA worker, she believes that it is important to know and assert one’s rights. “Change will come only when ASHAs learn to say no to unequal treatment and stand up against it,” she told us in a detailed interview.
Without, But Also Within
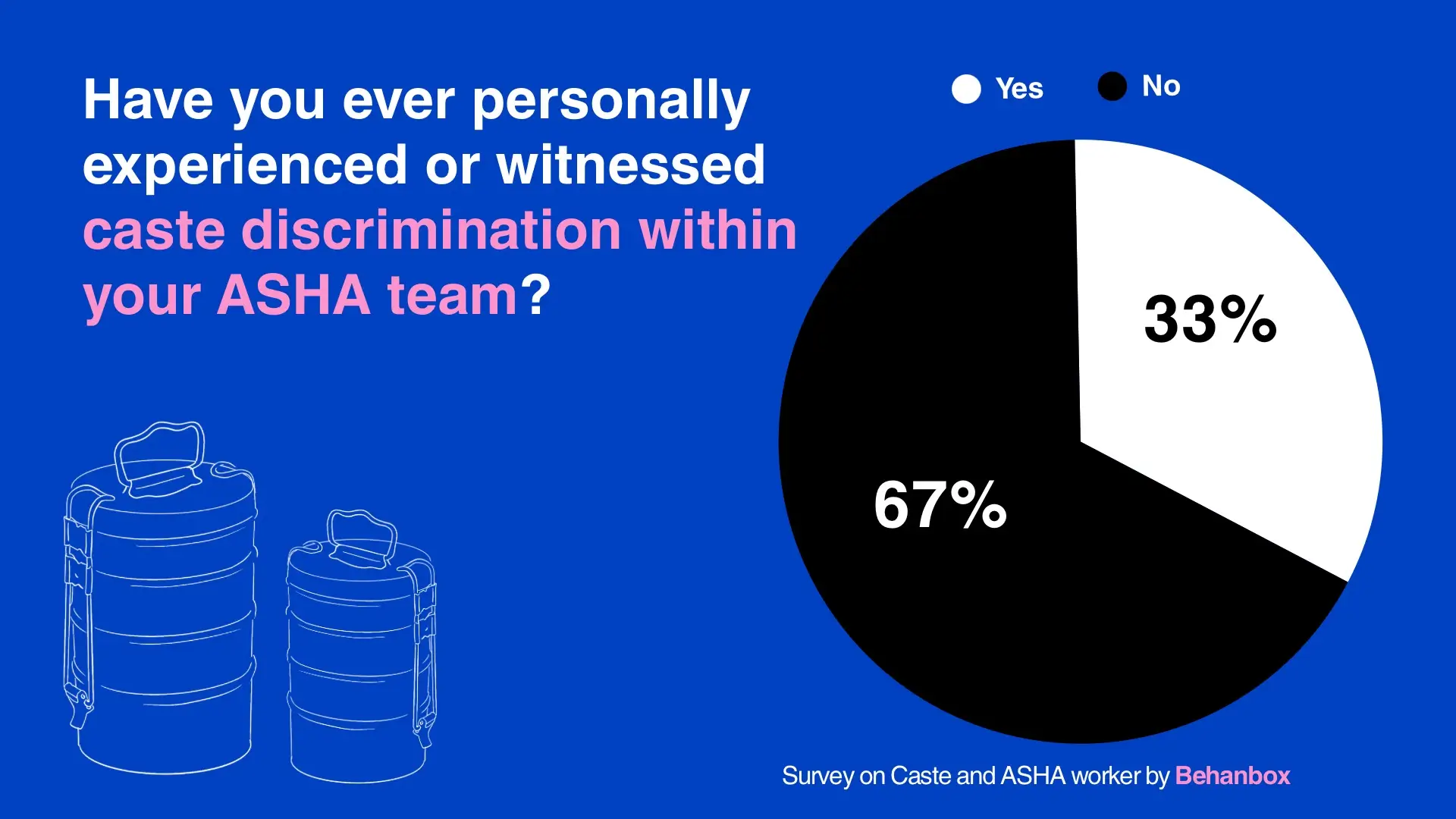
Caste also defines how Scheduled Caste ASHA workers navigate their relationship with fellow ASHA workers and other staff members at the local health centres. Around 33% of SC ASHA workers in our survey shared that they have experienced or witnessed at least one instance of caste discrimination within their team.
In 2007, Kaushalya Devi, 43*, an ASHA worker from Jungle Nahar Chhapra village in Kushinagar district of Uttar Pradesh, confronted an upper caste ASHA worker during a meeting over casteist remarks. Back then, casually asking an ASHA worker her caste was as common as asking her name.
“When I said I am a Chamaar, a Mishra (Brahmin) woman remarked, ‘Accha, aapke husband joote silte hain (okay, so your husband mends shoes)?” Hurt, she retorted: ‘Accha…aap hi ke husband, hamare ghar gaye the bheek maangne? Aur ussi joote ki kamai se hum unko bheek diye the (oh, it was your husband who came begging at our door and my husband gave him alms from the money he earned by mending shoes)? Even today, the woman does not look me in the eye,” recounted Kaushalya.

Casteist remarks and other practices like untouchability often render workplaces unsafe and lonely for many SC ASHA workers. Sonara Alaji’s OBC ASHA colleague refused to share water despite working with her for three years though they were friends. And in her 16 years of service, Suman Kamble of Kolhapur said she never felt a sense of belongingness.
“They have their own group, chat among themselves and don’t involve me,” she told BehanBox. The only ASHA worker who shares her food is Muslim.
Lakshmi, the ASHA facilitator from Madhya Pradesh said that upper caste ASHA workers do not engage with them outside work, never, for instance, attend functions at their home. She recalled that upper caste ASHA workers had refused to attend a wedding in the family of an SC ASHA facilitator. “The same women attended my daughter’s wedding, ate and enjoyed it,” said Lakshmi.
Sneha Kumari from Bihar pointed out how even ASHA workers from the backward castes also covertly exercise authority over SC ASHAs, for instance, asking them to take on petty tasks. She said never complied but those who did continued to be oppressed.
Sometimes, SC ASHA workers are called in to access areas where upper caste ASHAs refuse to or are not allowed to go by their families. Sneha Kamble said that, when in need, she would rather reach out to an SC ASHA worker from another village than her own.
Our interviews showed that Dalit ASHA workers tended to be more mobile and independent. Upper caste women, Lakshmi said, are more restricted by notions of ‘purdah’ and patriarchy while SC ASHA workers had no choice but labour. When she entered her home after visiting Dalit communities her mother-in-law would demand that she bathe first. “We were also treated like untouchables in our own home,” she pointed out.
These caste-coded social norms often restrict the participation and mobility of Scheduled Caste ASHAs, even without explicit enforcement. The presence of SC facilitators can be empowering and supportive. But there is little organised or collective opposition to casteism within the ASHA system.
ASHA Unions and Caste Question
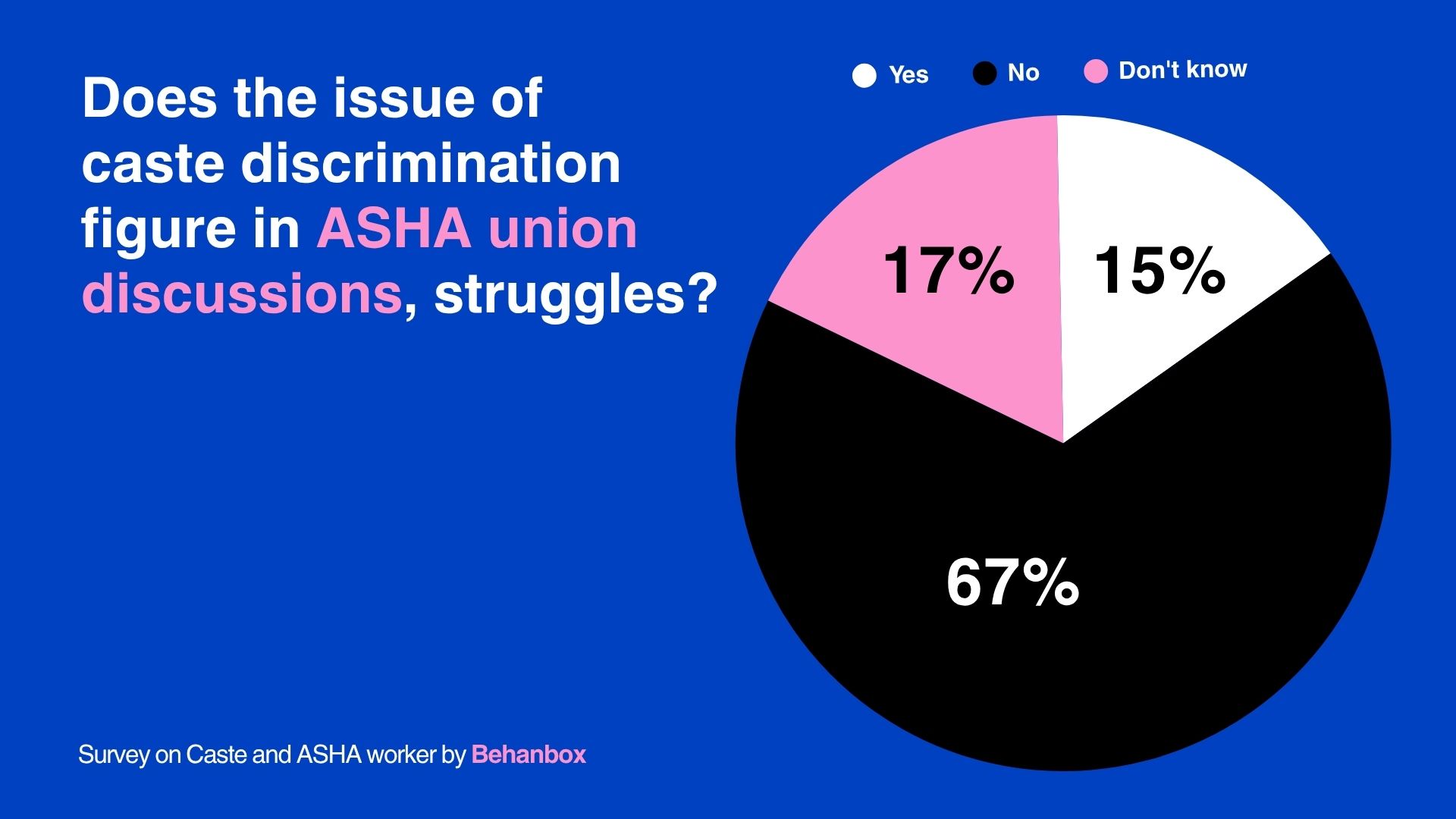
Caste follows Scheduled Caste ASHA workers into union spaces too. As many as 67% of ASHA workers in our survey said that caste does not figure in ASHA union meetings or discussions.
Prerna*, a Scheduled Caste ASHA worker from Haryana’s Palwal district and district president of the Centre of Indian Trade Unions (CITU), has been organising ASHA workers since 2009. While she has consistently raised labour issues on public platforms, she too has endured caste prejudice.
“I noticed that some people I worked with were more concerned about how we looked and dressed, and believed we were not ‘presentable’ enough,” Prerna said, adding that it took three years of unionising work to earn respect from others. Even today, some upper caste peers—both ASHA workers and union leaders—continue to put her down with comments that her looks are “simple” or that she is “not photogenic enough”.
When a health worker is denied something as basic as a chair or clean drinking water, it becomes a question of the right to dignity and equal working conditions.
Avani Chokshi, labour lawyer with the All India Central Council of Trade Unions (AICCTU), argued that the core problem lies in the State’s refusal to recognise ASHA workers as employees and instead designate them as volunteers. Recognising them as government employees would guarantee them minimum workplace rights, including access to drinking water, seating, safe working conditions, and protection from discrimination.
Labour lawyer and member of Lawyers Collective Sanober Keshwar argues that labour laws in India remain “completely caste-agnostic”, focusing largely on economic entitlements such as wages, bonuses, gratuity, and pensions. In doing so, they fail to address the dignity and lived realities of workers, apart from limited protections under laws on workplace sexual harassment.
Instances of “discrimination and injustice” were addressed individually, but caste discrimination was never treated as a central political issue or discussed seriously in larger union meetings, said Lakshmi Kaurav and Netradeepa Patil, both from dominant caste communities.
“We have not had any large-scale discussion on this because there have been no major cases reported,” said Netradeepa. “ASHA workers often do not speak up, as they see it as a personal issue. But we are trying to include members from all communities so that everyone feels equal.”
‘Need To Fight For Wages, But Also Dignity’
Lakshmi has organised meetings across villages on issues such as child marriage, restrictive social customs like the compulsory ghunghat, but caste is often ignored because it is considered “unimportant”. And those who staunchly believe in casteist practices, she added, are not ready to change.
Caste prejudice also surfaces during union-led protests, particularly when ASHA workers travel across districts. For instance, some upper-caste ASHA workers would refuse to attend meetings if it required waiting at a SC colleague’s home during transit.
“Didi, they clean the latrines. Don’t take us to such places unless you know where we will be staying,” an upper-caste ASHA worker told Lakshmi in 2023, after an overnight stay at a Valmiki ASHA worker’s home.
Since then, Lakshmi has adopted a “no questions asked” approach, asking ASHA workers to accompany her only if they are willing to stay wherever food and basic sleeping arrangements are available. “Those who still have problems don’t come along,” she says.
Srujana argued that a higher honorarium is important but it will not end caste discrimination. For that it is critical that internal social hierarchies be confronted.
“Wages may be the same for all ASHA workers, but experiences are not. Caste fragmentation produces unequal working conditions, which are then normalised,” she said. She further called for intra-workforce accountability mechanisms and collective platforms that cut across caste lines.
There is general reluctance among Dalit workers to raise issues of discrimination at union meetings and those among them who try to take up leadership roles are not heard seriously enough, said Sneha. For Prerna, who holds a position of leadership, her ASHA peers are a ‘family’, and fighting for their rights is what sustains her. She had left the union briefly, upset by the casteist remarks of some colleagues, but was convinced by others to return. She is driven, she said, by the need to highlight the challenges faced by ASHA workers from marginalised and caste oppressed communities.
“They feel encouraged seeing us. I do not want to break their hope or expectations. When they feel inspired and learn something, I choose to ignore these issues,” said Prerna.
*Some names have been changed to protect identity.
The data behind this investigation comes from a survey of 52 SC ASHA workers across six states: Bihar, Gujarat, Uttar Pradesh, Haryana, Rajasthan and Maharashtra. To request the cleaned dataset for research, advocacy or reporting, fill this form.
A brief note on the survey methodology
The survey was conducted with 52 ASHA workers from SC communities across 6 states– Bihar, Gujarat, Uttar Pradesh, Haryana, Rajasthan and Maharashtra. The survey was conducted both in-person and through telephonic interviews. We surveyed 13 SC ASHA workers on the field and 39 on the phone.
The survey had 19 questions. These included their demographic, education and caste details. The questions on the experience of casteism within the healthcare system included instances (if even one time) of caste discrimination, detailed narration of the experience, institutional support mechanisms, questions on bribery and favoritism, opportunities and upward mobility, mental health effects and spaces within the labour unions. These responses were then converted to variables and analysed.
One major shortcoming of the survey is that it was conducted in Hindi speaking regions, leaving the entirety of South India and many other states due to resource constraints. We hope this is a start into a longer research and inquiry into the caste question in other states.




We believe everyone deserves equal access to accurate news. Support from our readers enables us to keep our journalism open and free for everyone, all over the world.
