More Women, Adivasis, Dalits and Muslims Died During COVID-19 First Wave
Unlike the rest of the world, women’s life expectancy fell by more years than men’s and that of marginalised communities fell more sharply in the first year of the pandemic. This skew, say, researchers can be traced to social inequalities
- Swagata Yadavar

There were 1.19 million excess deaths in India in 2020, more eight times the official COVID-19 death count and 1.5 times the WHO’s extrapolated estimate, said a new paper published in Science Advances, an open-access multidisciplinary journal by American Association for the Advancement of Science.
Excess deaths are calculated by comparing the total number of deaths in a pandemic year with the total number of deaths in a year without a pandemic event.
There were 17% more deaths in 2020 compared to 2019, the paper found. These deaths led to a reduction of 2.6 years in life expectancy at birth for Indians. Women in India experienced a life expectancy decline of 3.1 years at birth, a year more than for men (2.1 years). Excess deaths in different age groups leads to reduction in life expectancy at birth for a population.
This number is in contrast to the patterns observed in almost every other country in the world where more men died during COVID-19 than women. This can be attributed to gender inequality in India, wrote researchers from the University of Oxford, University of California Berkeley, University of Texas, Austin, Emory University and others.
India’s official COVID-19 death toll from 2020-2024 was 533,540 while the US with the most casualties stood at 1.12 million deaths.
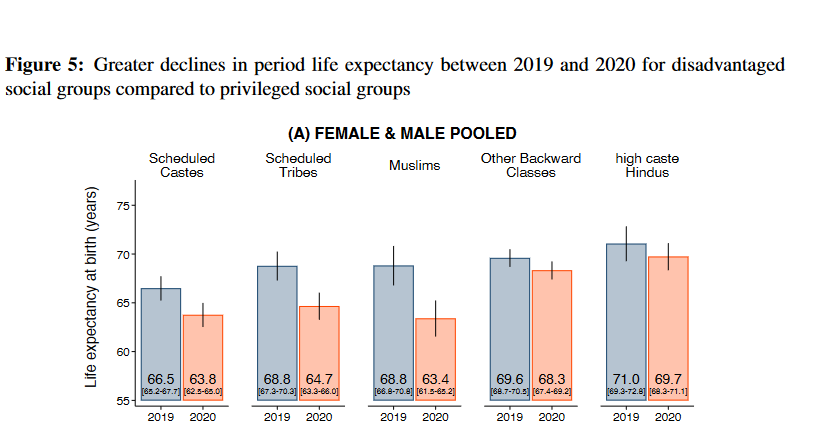
The toll of the pandemic was experienced unevenly in India — marginalised social groups — Muslims, Scheduled Tribes and Scheduled Castes experienced greater declines in life expectancy than high caste Hindus. “Larger decreases among marginalised groups increased already stark disparities,” the authors wrote.
This is the first study that examines the mortality impacts of the pandemic by sex, social group and age and it was done using data representative of one-fourth of India’s population from the National Family Health Survey (NFHS)-5. The authors used the NFHS survey’s mortality data from 11 states from 2021 to estimate the deaths in 2020 during the first wave of the pandemic.
“We can’t rely on the Civil Registration System dataset to understand gender or social inequality in mortality figures,” said Aashish Gupta, a Marie Skłodowska-Curie Fellow at the University of Oxford and co-author of the paper. “It [civil registration] is incomplete and women’s death registration levels are even lower than men and caste is not captured. The NFHS meanwhile has a long history of estimating mortality well and captures information on caste and gender.”
India’s civil registration system does not capture all the deaths. Also, death registrations rates vary from 13.5% in Arunachal Pradesh to 98.8% in Punjab and only 39.8% of women’s deaths are registered.
More Female Than Male Deaths
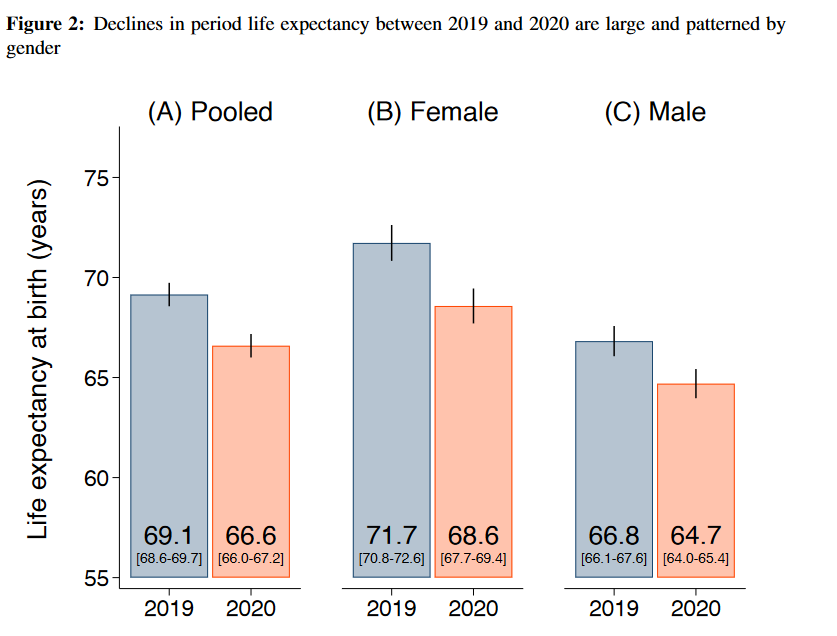
The life expectancy at birth in India fell from 69.1 years in 2019 to 66.6 years in 2020.
Declines in life expectancy were recorded across the world after COVID-19 pandemic, including in high income countries. For example, life expectancy at birth fell by 1.5 years in the US (from 78.8 years in 2019 to 77.7 years in 2020) and by 1.6 years in 2020-22 across the world.
While the life expectancy declines were driven by deaths of those above 60 years in high income countries, in India the decline was among the youngest and the older groups. This was higher than the seroprevalence recorded in India and could be due to the indirect effects of the pandemic, the paper noted.
The life expectancy of women at birth in 2019 was 71.7 years which fell to 68.6 years in 2019, a reduction of 3.1 years while the life expectancy of men in 2019 was 66.8 years which declined to 64.7 years in 2020, a reduction of 2.1 years.
“Such a large female disadvantage in the impact of the pandemic as observed in India has not been documented in any country,” the paper noted. It further noted that this was observed even in civil registration data and was observed in all social groups and reflects gender inequality in the country.
Earlier research showed that Indian households spend less on women than men and this could have worsened during the pandemic, the authors noted.
Muslims, Marginalised Groups vs Upper Caste Hindus
The paper found marginalised groups experience the largest reductions in life expectancy at birth — while high-caste Hindus lost 1.3 years in life expectancy, the loss for Muslims was 5.4 years, for STs 4.1 years and for SCs 2.7 years. The decline for OBCs was similar to that of high caste Hindus.
Previous studies had shown, compared to upper caste Hindus, Adivasis, Dalits and Muslims already had a shorter life expectancy at birth.
The Muslim life expectancy was lowest across the five groups and was consistent with the marginalisation of Muslims in 2020 with greater increase in neonatal mortality, the paper noted.
Similar reduction in lifespans was experienced among Blacks (3.3 years), Hispanics (4 years) and Native Americans (4.5 years) in the US in 2020 as compared to 2019 according to the National Centre for Health Statistics . However, the declines in India were at higher relative magnitude as the life expectancy for these groups were already low in 2019 — 66.5 years for Scheduled Castes and 68.8 years for Scheduled Tribes and Muslims.
This skew is due to the substantial discrimination, exploitation, and violence faced by marginalised groups, said Murad Banaji, departmental lecturer in Applied Mathematics, University of Oxford and co-author of the paper. “In addition to inequalities in access to healthcare and discrimination in health settings, social conditions, such as those related to exposure to hazardous work, physical violence, poor access to nutrition, and denial of equal opportunities contribute to major life expectancy disparities,” he said in an email interview.
This paper gives an indication of the scale of India’s COVID-19 casualties although it does not capture the deaths during the Delta wave of 2021 which recorded higher mortality. It however dispels claims made by the Indian Prime Minister Narendra Modi and other ministers that the ‘Indian government’s health response was the best in the world and helped save large scale casualties’.
“The severe undercounting of pandemic deaths in India seems to be a result of two factors: weak systems for recording deaths; and deliberate efforts to ‘manage’ the data by governments, at both local and national level,” said Banaji.
Methodologically, this study shows the potential for accurately estimating mortality, even for short periods, using household survey data which would be helpful for routine mortality surveillance and future mortality crises. “We also hope that this study brings a greater focus to disadvantaged groups including females, marginalised populations, and rural areas in understanding and responding to future pandemics,” said Sangita Vyas, Assistant Professor in Economics at CUNY Hunter College and co-author of the paper.
This kind of study shows that when there are other forms of data available, we get a more reliable source of deaths than just the civil registry system, said public health expert Dileep Mavalankar, former director of Indian Institute of Public Health, Gandhinagar. His study on excess mortality during heat waves in 2010 led to widespread policy action and the implementation of a heat action plan in Ahmedabad.
“India has not been collecting or publishing daily all-cause mortality data which leads to severe undercounting of deaths especially of the vulnerable groups,” he said. This undermines health priorities and leads to a false sense of complacency and smaller health budgets, he added.
India’s Union health budget’s spending as a percentage of its GDP has been falling since the pandemic – from 0.56% in 2021-22 to 0.42% in 2022-23 to 0.35% in 2023-24 reflecting the government’s priorities.
India also delayed releasing or not conducting crucial data surveys such as the Census, socio-economic caste census, household consumer expenditure survey, medical certification of cause of death data among others.
There needs to be legislation to make health and hospital data public regularly, “Health data is like a pulse of the people – if we don’t know the pulse, how can we tell if the patient is alive and well?” Mavalankar said.

We believe everyone deserves equal access to accurate news. Support from our readers enables us to keep our journalism open and free for everyone, all over the world.
